Exam of the Lower Extremities
The discussion which follows focuses on the search for evidence of arterial and venous insufficiency as well as edema. These are the most common serious ailments which affect the lower extremities and therefore merit the greatest attention. Joint and neurologic examinations are covered elsewhere.
The Femoral Region:
As with examination of any other area of the body, exposure is key. Socks, stockings, pants and skirts should all be removed.
- Begin by simply looking at the area in question, which is on either side of the crease separating the leg from the groin region. Make note of any discrete swellings, which might represent adenopathy or a femoral hernia.
- Palpate the area, feeling carefully for the femoral pulses as well as for inguinal/femoral
adenopathy (nodes which surround the femoral artery and vein.... up to one cm in size are
considered non-pathologic). If you feel any lymph nodes, note if they are firm or soft,
fixed in position or freely mobile (fixed, firm nodes are more worrisome for pathologic
states).
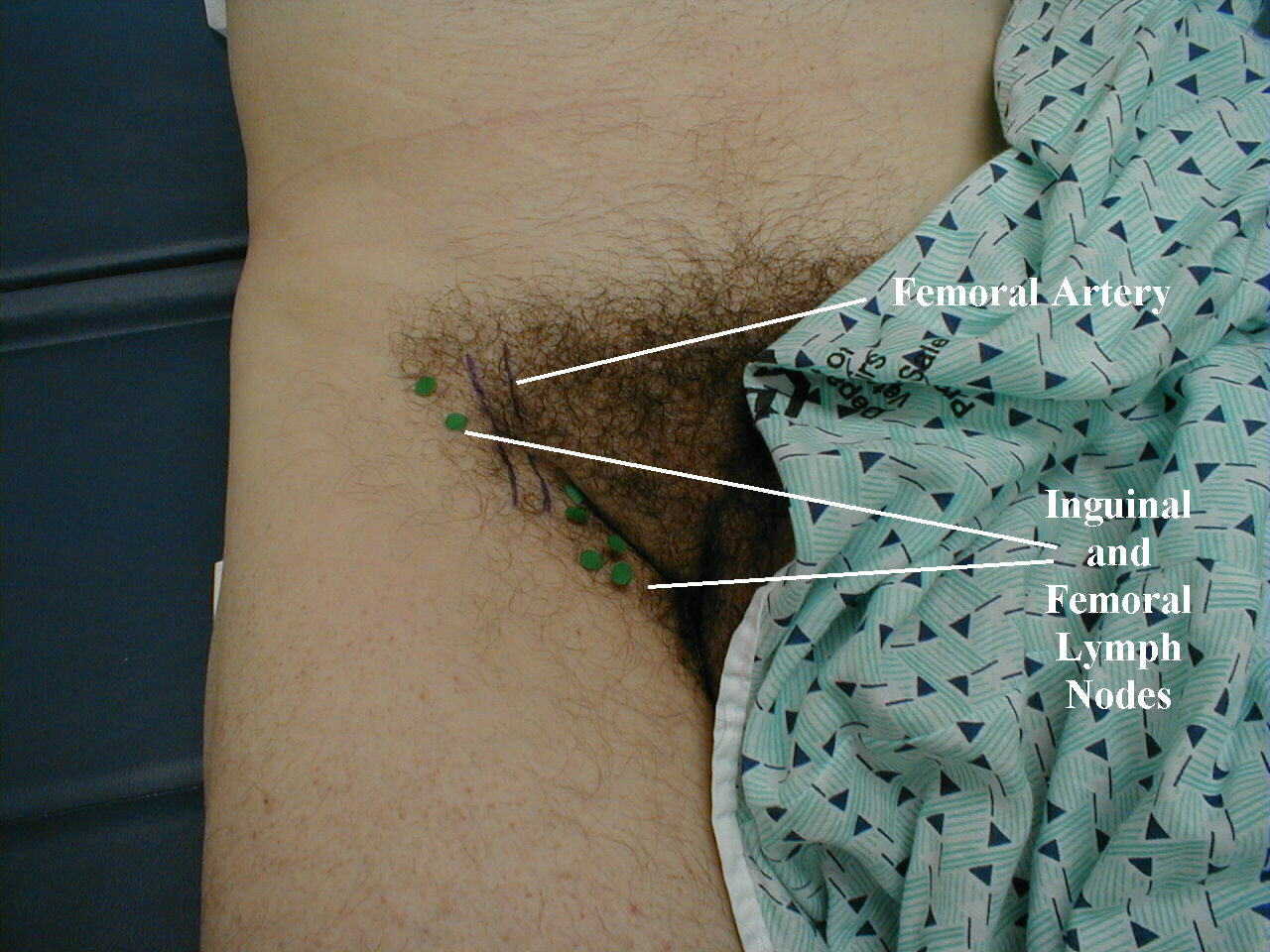

- The femoral pulse should be easily identifiable, located along the crease midway between the pubic bone and the anterior iliac crest. Use the tips of your 2nd, 3rd and 4th fingers. If there is a lot of subcutaneous fat, you will need to push firmly.
- A femoral hernia, if present, is located on the anterior thigh, medial to the femoral artery. As it can be transient (i.e. the patient reports its presence yet you find nothing on examination), investigation should include observation as well as palpation while the patient performs a valsalva maneuver, which may make a hernia more prominent.
The Popliteal Region:
- Move down to the level of the knee allowing it to remain slightly bent.
- Place your hands around the knee and push the tips of your fingers into the popliteal fossa in an effort to feel the popliteal pulse. Note whether it feels simply pulsatile (normal) or enlarged and aneurysmal (uncommon). This artery is covered by a lot of tissue and can be difficult to identify, so you may need to push pretty hard. Even then, it may not be palpable, which is not clinically important if you can still identify the more distal pulses (see below).


Below The Knee: Now, turn your attention to the lower leg (i.e. from the knee to the foot). First, examine with your eyes, paying attention to:
- Color: Venous insufficiency is characterized by a dark bluish/purple discoloration. Over
time, long standing stasis of blood leads to the deposition of hemosiderin, giving the skin
a dark, speckled appearance. If the leg is placed in a dependent position, the bluish/purple
discoloration may darken dramatically, further suggestive of venous insufficiency. This
occurs as a result of gravity working against an already ineffective blood return system.
Patients with severe arterial insufficiency, on the other hand, may have relatively pale
skin as a result of under perfusion. When their legs are placed in a dependent position,
gravity enhances arterial inflow and the skin may become more red as maximally dilated
arterioles attempt to bring blood to otherwise starved tissues. In cases of severe ischemia,
the affected areas (usually involving the most distal aspect of the foot), can appear
whitish or mottled, giving the leg a marbleized appearance. Dead tissue turns black (a.k.a.
gangrene). Cellulitis (infection in the skin) will cause the skin to appear bright red.
These changes can be difficult to detect in people of color.
Acute Arterial Insufficiency:
Note Mottled Appearance of Skin Chronic Arterial Insufficienc with Ulcers
Chronic Arterial Insufficienc with Ulcers Gangrene of Toes
Gangrene of Toes Venous Insufficiency
Venous Insufficiency Cellulitis
Cellulitis
- Obvious swelling of the leg: If present, is it symmetric? To what level does the swelling
exist
(i.e. ankle, calf, knee etc.)?
Assymetric Leg, Swelling secondary to Deep Venous Thrombosis in Right Leg.

- Nail growth: Nail thickening and deformity often occurs with arterial insufficicency; also
with fungal
infections.
Onychomycosis

- Skin: Any obvious growths? Shiny, hairless appearance (seen with arterial insufficiency)?
Dilated or varicose superficial veins? Ulceration of the skin can occur in the setting of
either
venous or arterial disease.
Venous Stasis Ulcer

- The bottom of the foot and between the toes: These are common "problem areas," particularly
in patients with diabetes who are predisposed as a result of sensory impairment, arterial
insufficiency, or both.
Neuropathic Ulcer in Patient
with Diabetic Neuropathy
- Probing the depth of an ulcer: Ulcers can extend rather deeply. This can
be explored with the use of a Q-tip. If the bone is visible or can be reached
with the Q-tip, the infection is assumed to involve the underlying structure.
This is referred to as clinical osteomyelitis. It's worth noting that if the
ulcer developes in a patient with neuropathy (as is the case here), then the
act of probing does not cause pain because the area is insensate.
Clinical Osteomyelitis:Deep ulcer which permits passage of Q-tip to underlying level of bone.

Feel the skin, noting in particular:
- Temperature: Arterial insufficiency will often cause the skin to feel cool. Infection, on the other hand, causes hyperemia and relative warmth. The back of your hand may be the most sensitive surface for detecting subtle temperature difference. Compare one leg to the other. It's also OK to use your own skin (e.g. face) as a reference point. Note that in cases where arterial insufficiency and infection occur simultaneously (which is quite common), impaired inflow of blood may generate less warmth (and also less redness) then might otherwise be expected.
- Edema: Fluid frequently collects in the feet and ankles due to the effects of gravity. This
is related to some perturbation in the Startling forces. Thinking in broad strokes, it's
usually the result of:
Low oncotic pressure: Either failure to synthesize albumin (as with malnutrition or liver disease) or increased loss of albumin (via the kidney or local leakage due to altered capillary permeability).
Increased hydrostatic pressure: Transmitted back from the level of the heart (right heart failure), liver (portal hypertension), local venous insufficiency (e.g. venous valvular incomepetence with impaired flow of blood back to the heart from the legs), lymphatic obstruction (e.g. retroperitoneal adenopathy secondary to malignancy), or obesity (which may impair both venous and lymphatic drainage).Realize that all "circulation" problems are not the same. Disorders of blood inflow (arterial) and outflow (venous) have different associated signs and symptoms based on their varying pathophysiology (see above). Edema is commonly associated with venous insufficiency, a blood return problem. This disorder tends to get worse when the legs are allowed to dangle for prolonged periods below the level of the heart (e.g. towards the end of the day if the patient has been standinag for long periods of time). The fluid builds up preferentially in the most distal aspects of the leg and progress up towards the knee as the process worsens. Arterial insufficiency, on the other hand, rarely causes edema, which makes perfect sense as the problem lies in the delivery of blood to the extremity, not the return from it. On occasion, the conditions may coexist.
It may be difficult to detect small amounts of fluid. Look around the malleoli, as fluid will cause a loss of the normally distinct appearing edges of the bone. Similarly, fluid will tend to "fill in" the spaces between the extensor tendons on the top of the foot, causing them to appear less defined. If you're not sure whether fluid is present, push on the area for several seconds, release, and then gently rub your finger over that same spot, feeling for the presence of a "divot," referred to as pitting. Much is said about pitting edema being associated with some disease states and non-pitting with others; however, the actual importance of this distinction is probably over stated. Also note the proximal extent of the edema and if it is present to the same degree in both legs. Edema may either be diffuse, involving all of the surrounding tissue symmetrically, as is frequently the case in disorders of low oncotic or elevated hydrostatic pressure. If, however, there is a local inflammatory process, as might occur with cellulitis, the area of edema can be quite focal. There is a very subjective scale for rating edema which ranges from "trace at the ankles" to "4+ to the level of the knees." After examining many patients, you'll develop a sense of what is a lot and what is not.
For Additional Information See: Digitial DDx: Edema
Edema can also be quantified by estimating of the depth in millimeters of the “divot” left after applying steady pressure to the skin, best done over the tibial region. A comparison of the different ways of quantifying edema are demonstrated here:
Quantifying Edema
 Normal
Normal 2+ edema - extending to above ankle
2+ edema - extending to above ankle 4+ edema – extending to upper tibia
4+ edema – extending to upper tibia1+ Minimal Barely detectable impression 2mm 2+ Mild Slight indentation 4mm 3+ Moderate Deeper indentation 6mm 4+ Severe Very deep indentation 8mm *Changes in Weight Very Helpful Clinically for Assessing Total Body Volume and impact of Diuretics*  Lymphedema, Left Leg
Lymphedema, Left Leg
- Capillary Refill: Push on the tip of the great toe or the nail bed until blanching occurs. Then release and note how long it takes for the red color to return, a reflection of blood inflow to the distal aspect of the lower extremity. Longer then 2-3 seconds is considered abnormal and consistent with arterial insufficiency. Refill may also be delayed in the setting of significant hypovolemia, as decreased blood volume available for perfusion is shunted away from the extremities to feed more vital organs.
- Skin that is discolored from venous insufficiency blanches when pushed and it generally takes more then a few seconds for the bluish hue to return. Cellulitic areas, however, blanch and then very rapidly return to their bright red coloration. This can be helpful as it will occasionally be difficult to determine if infection and venous insufficiency are both present.
- Pain: Cellulitic skin, for example, is often tender when touched. Remember that certain
disease
states (diabetes in particular) cause a peripheral neuropathy that predisposes these
patients to the development of skin breakdown and subsequent infection precisely because
they have abnormal sensation in their distal extremities. In these cases, then, infection
may occur in the absence of pain.

 Paronychia: Infection of the skin medial and inferior to nail of great toe. Image on the right is post I&D.
Paronychia: Infection of the skin medial and inferior to nail of great toe. Image on the right is post I&D. - Note the character of any swollen area: Does it feel full of edema fluid? Is there a suggestion of a solid mass (uncommon)? Is there focal fluctuance, as would occur in an abscess?
For Additional Information See: Digital DDx: Nonhealing Wounds and Ulcers
The Distal Pulses:
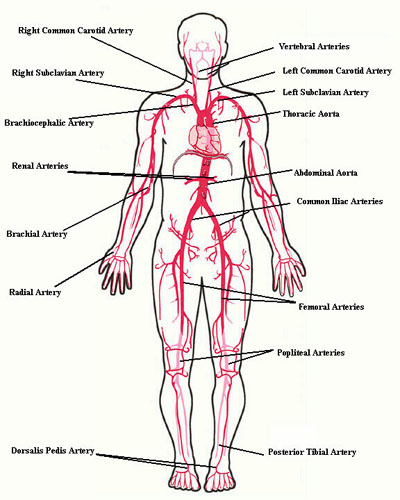
Pulses are assessed to identify the presence of arterial vascular disease. In general, the less prominent the pulses, the greater the chance that there is occlusive arterial disease. This is not a perfect correlation, however, as pulses may be palpable even when significant disease is present (e.g. may be affecting predominantly smaller, more distal blood vessels). A history of pain/cramps with activity suggestive of arterial insufficiency is also of great importance. The location of the blockage(s) will dictate the symptoms and findings. Aorto-iliac disease, for example, will cause symptoms in the hips/buttocks and a loss of the femoral pulse while disease affecting the more distal vessels will cause symptoms in the calves and feet.
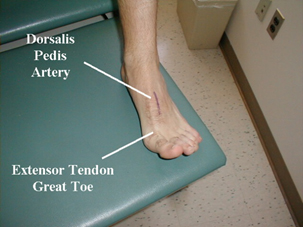
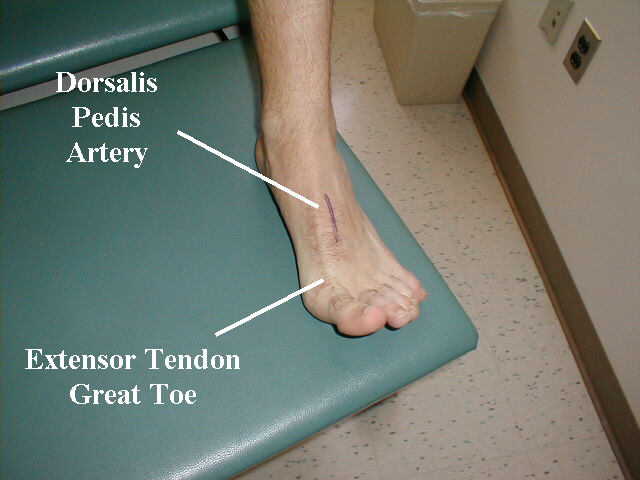
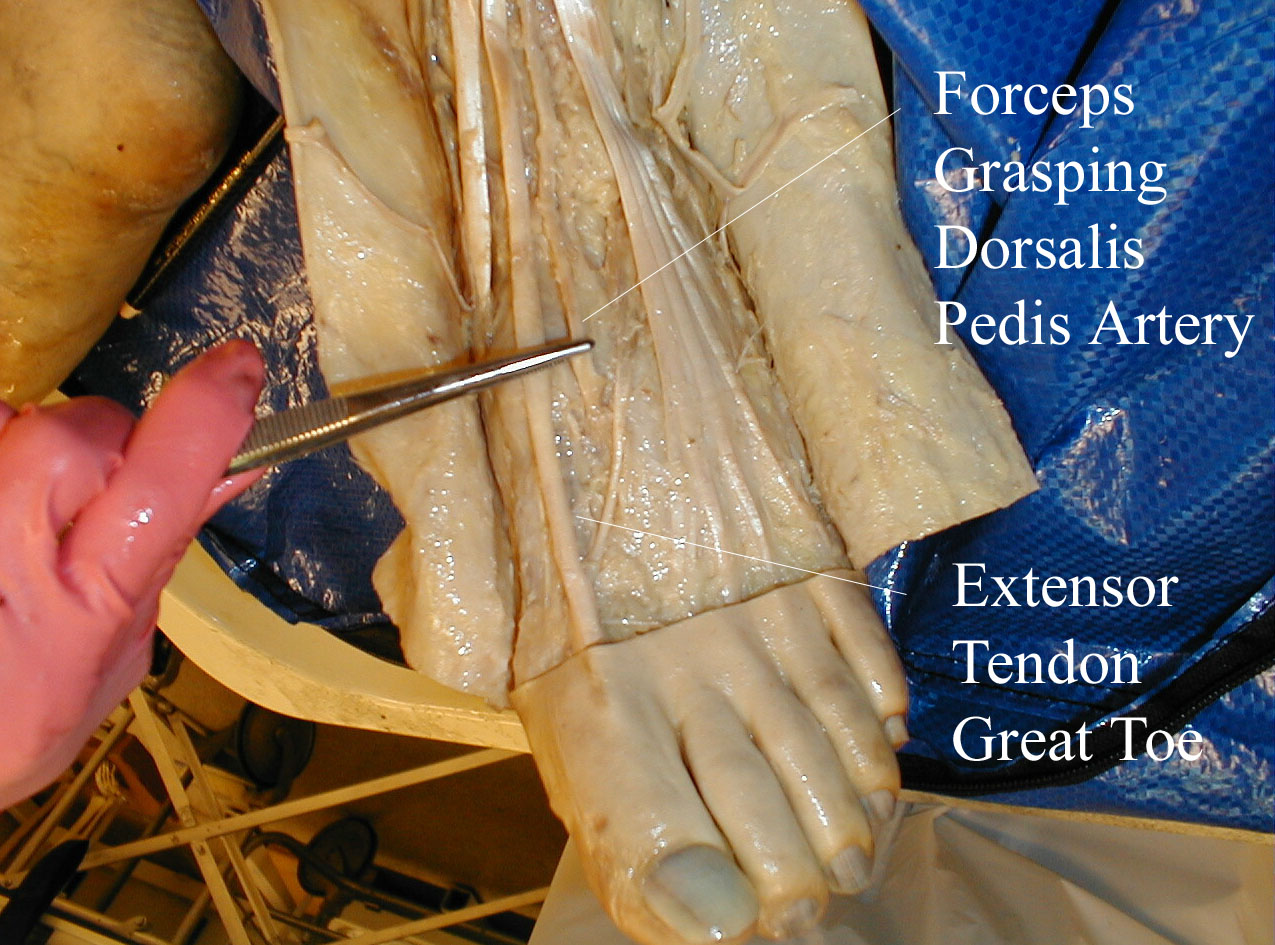
- The Dorsalis Pedis (DP) Artery: Located just lateral to the extensor tendon
of the big toe, which can be identified by asking the patient to flex their
toe while you provide resistance to this movement. Gently place the tips of
your 2nd, 3rd and 4th fingers adjacent to the tendon and try to feel the pulse.
If you can't feel it, try moving your hand either proximally/distally or more
laterally and repeat. Common pitfalls include pushing too hard and/or mistaking
your own pulse for that of the patient. Palpating the patients radial artery
or your own carotid simultaneously with your free hand can help sort this
out.
Location of Dorsalis Pedis Artery
The pictures below demonstrate the location of the dorsalis pedis artery in relation to surrounding structures (surface anatomy on left, gross anatomy on right).
 Palpating Dorsalis Pedis Artery Infection of the skin medial and inferior to nail of great toe. Image on the right is post I&D.
Palpating Dorsalis Pedis Artery Infection of the skin medial and inferior to nail of great toe. Image on the right is post I&D.
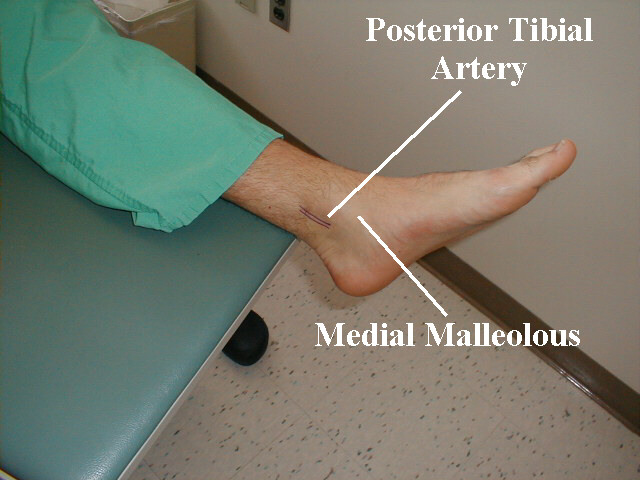
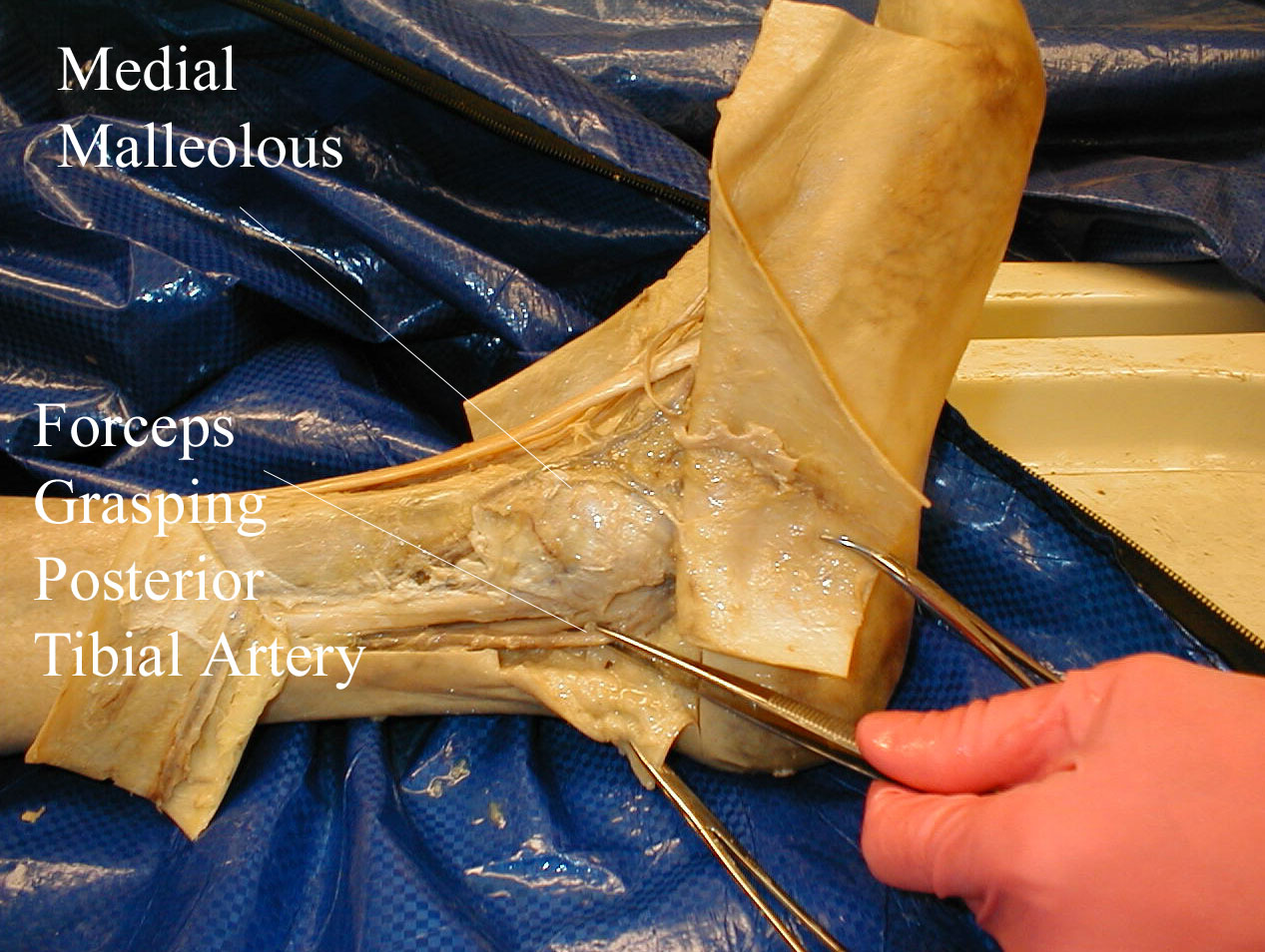
- The Posterior Tibial (PT) Artery: Located just behind the medial malleolous.
It can be palpated by scooping the patient's heel in your hand and wrapping
your fingers around so that the tips come to rest on the appropriate area.
Alternatively, you can reach your fingers over the top of the medial malleolous
and approach the artery from this direction. In either case, you are attempting
to locate the artery using the tips of your fingers. Pitfalls mentioned with
the DP also apply here.
Location of Posterior Tibial Artery The pictures below demonstrate the location of the posterior tibial artery in relation to surrounding structures (surface anatomy on left, gross anatomy on right).
 Palpating Posterior Tibial Artery
Palpating Posterior Tibial Artery
- If there is a lot of edema, you will have to push your way through the fluid-filled tissue to get down to the level of the artery.
- If you are unable to palpate a pulse, find a doppler machine, which should
be present on any inpatient floor or ER, and use it to identify the location
of the artery. Mark the place with a pen and then go back and again try to
feel it with your fingers. In this way, you will be able to determine if the
vessel was not palpable on the basis of limited blood flow or if you are simply
having a "technical" problem.
Using Doppler Device to Identify Posterior Tibial Artery

- Pulses are rated on a scale ranging from 0 (not palpable) to 2+ (normal). As with edema, this is very subjective and it will take you a while to develop a sense of relative values. In the event that the pulse is not palpable, the doppler signal generated is also rated, ranging again from 0 to 2+.