Musculo-Skeletal Examination
Shoulder Exam
For Additional Information See: Digital DDx: Shoulder Pain or Swelling
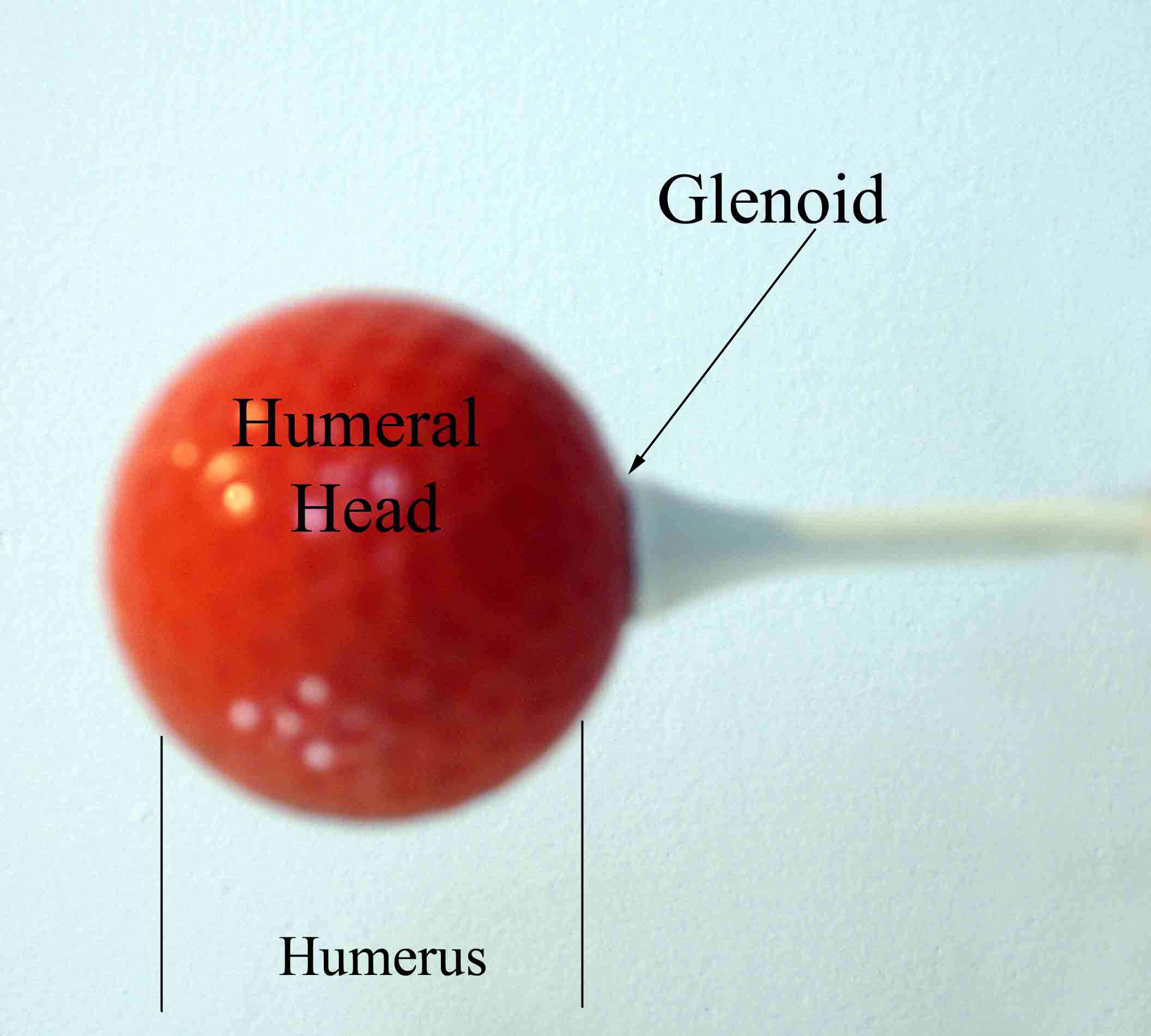
I think that the most daunting aspect of the shoulder exam is appreciating the functional anatomy of this incredibly mobile joint. The primary benefit of the ball and socket arrangement is that it allows the hand to be positioned precisely in space, maximizing our ability to function. In terms of functionality, the shoulder might be best described as having a golf ball-on-a-tee design.
Observation
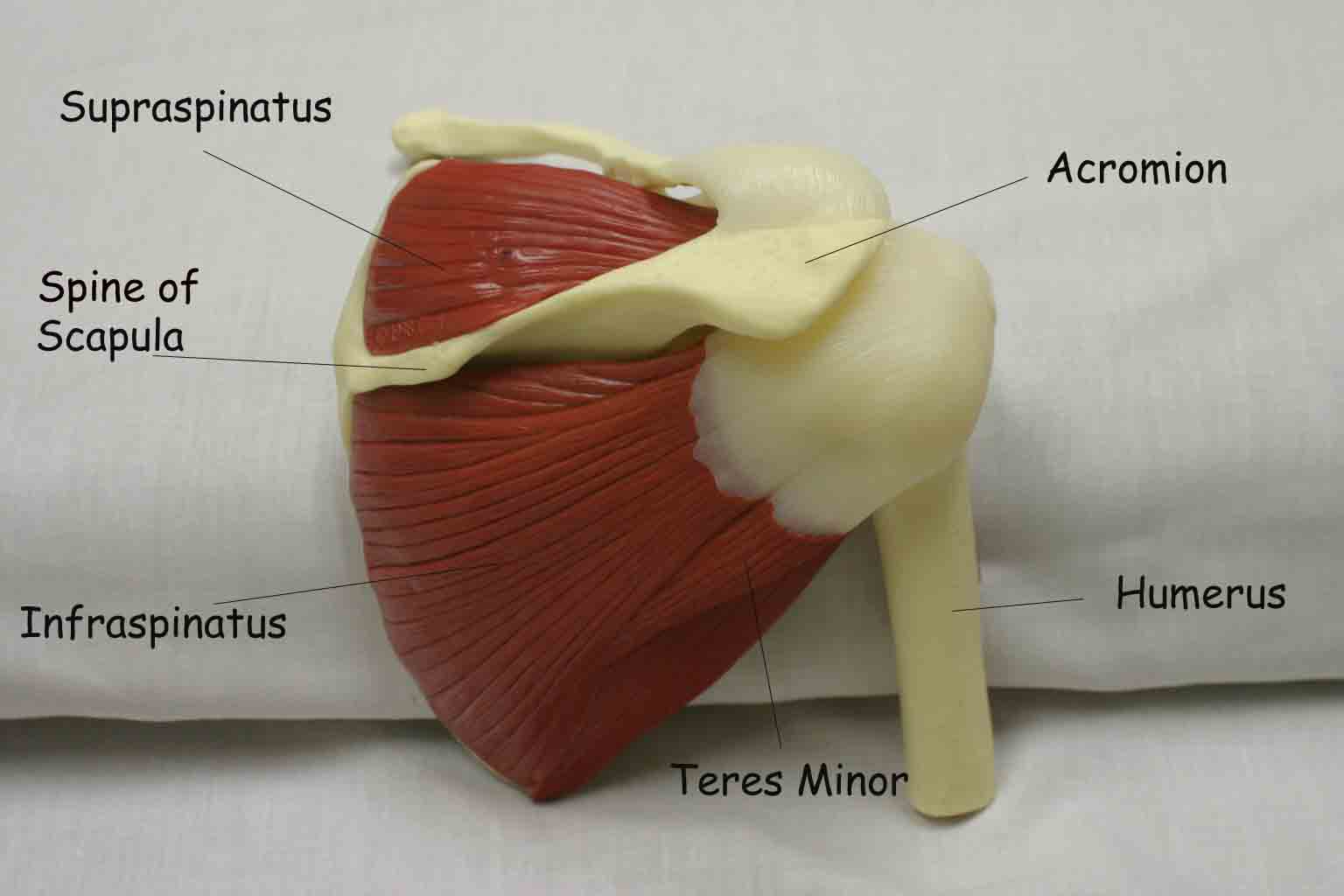
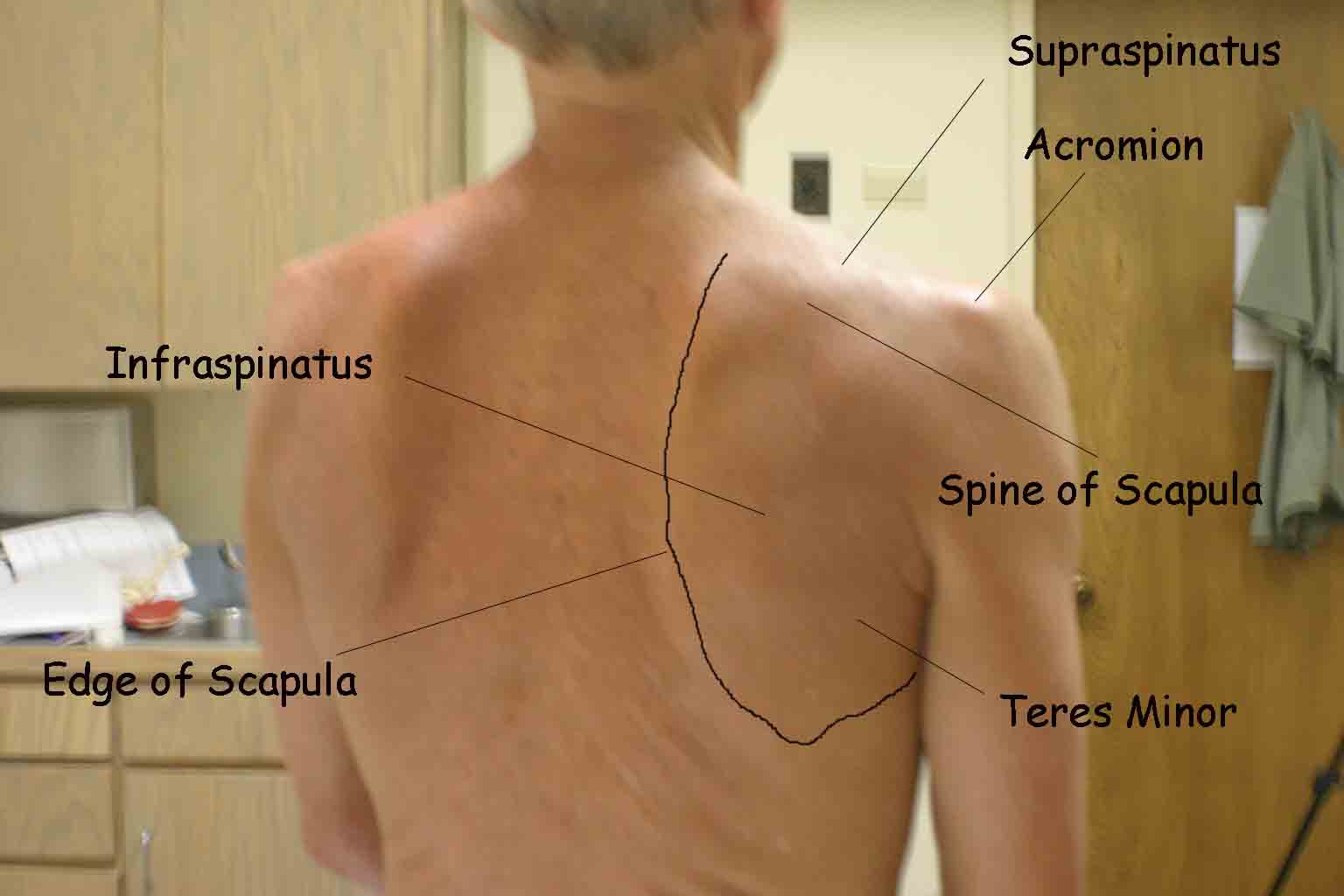
The shoulder joint is created by the confluence of 3 bony structures: the scapula, humerus and clavicle. These are held together by ligaments and an intricate web of muscles. Critical external landmarks include the following:
- Acromion
- Clavicle
- Scapula
- Deltoid muscle
- Supraspinatus
- Infraspinatus
- Teres Minor
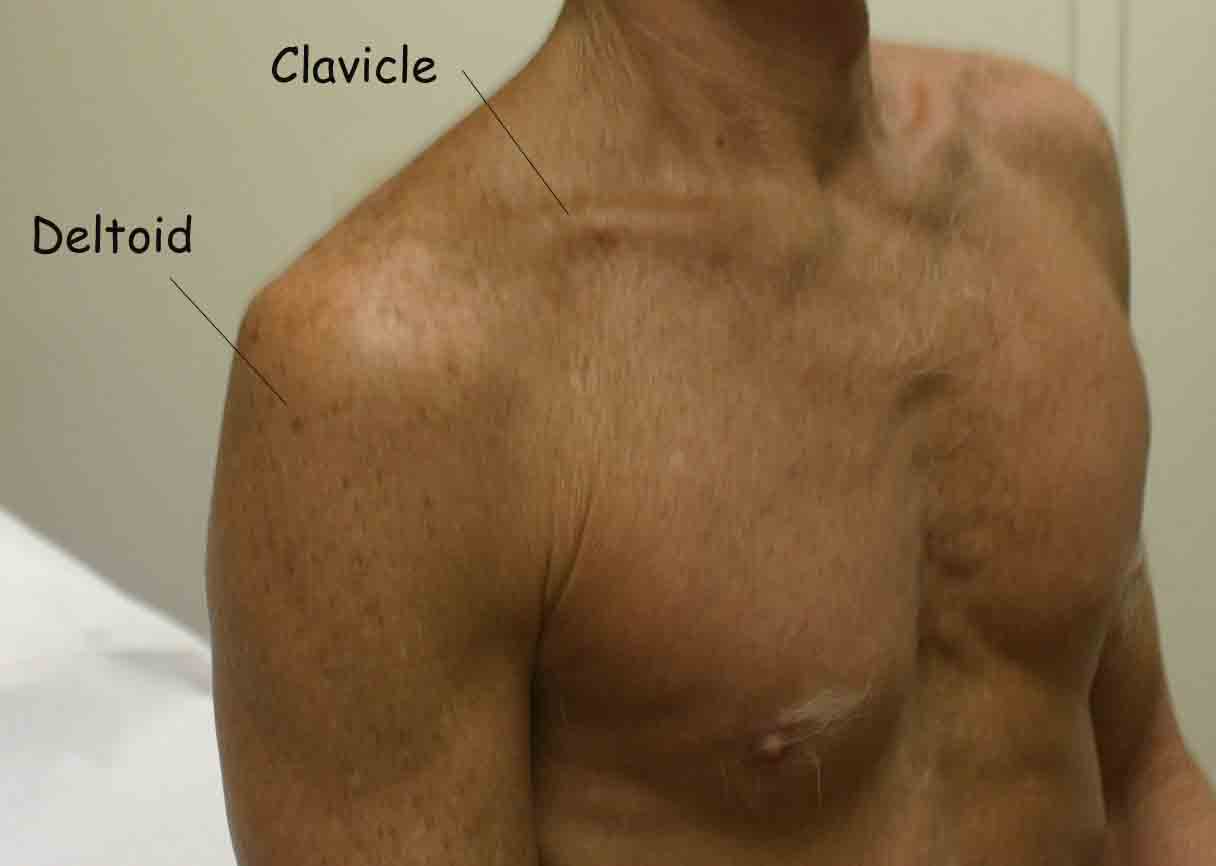
Start by looking at the normal (or more normal) side. Note any scars, obvious asymmetry, discoloration, swelling, or muscle asymmetry.
Palpation
Gently palpate around the shoulder, touching each of the landmarks noted above. Make note of pain.
Range of Motion (ROM)
If there are no symptoms, test both sides simultaneously. Otherwise, start with the normal side.
Active ROM:
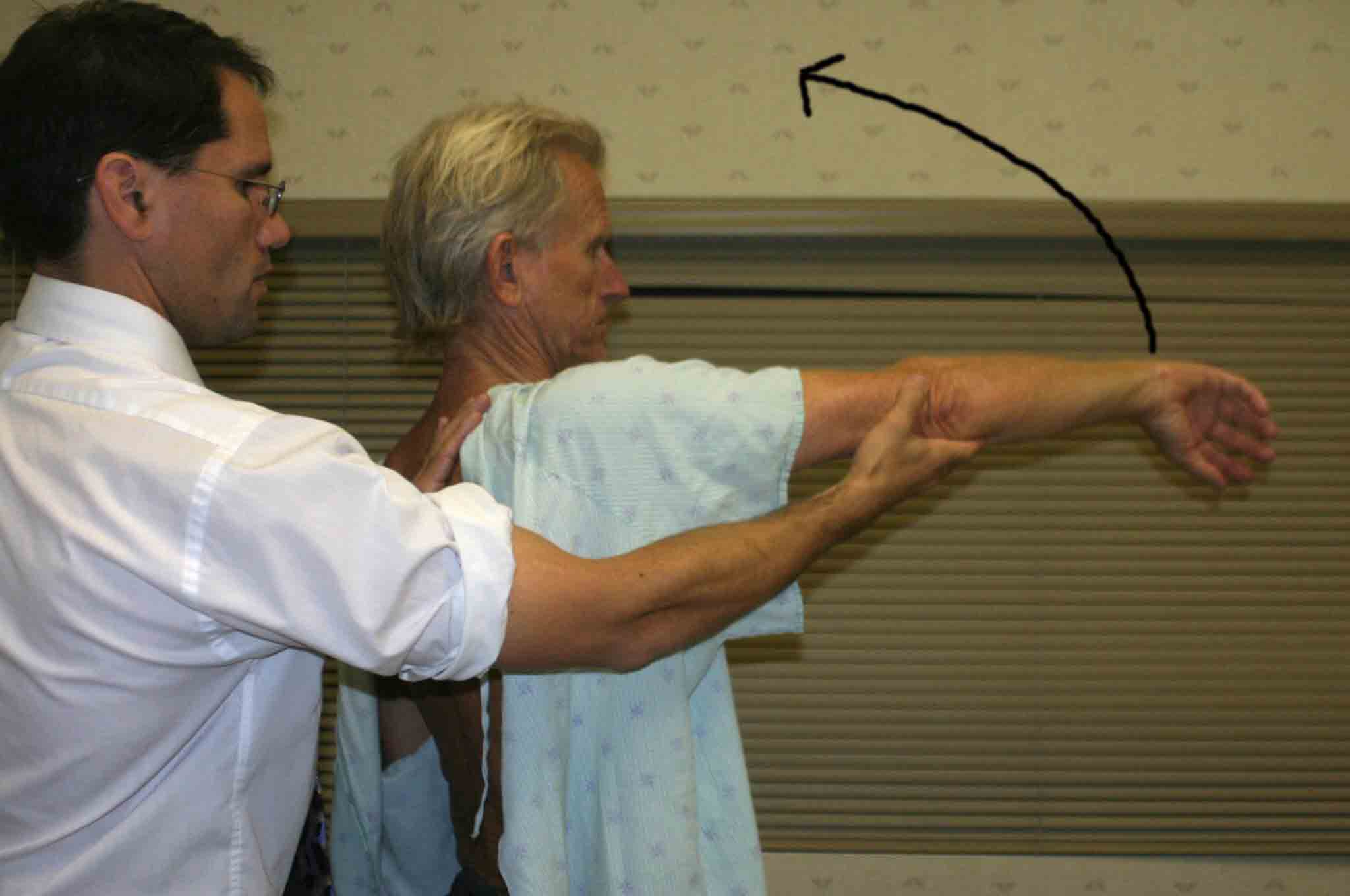
- Abduction: Determine the extent to which the patient can abduct
their arm. The patient should be able to lift their arm in a smooth, painless
arc to a position with hand above their head. Normal range is from 0 to 180
degrees.

- Adduction and Internal rotation (Appley Scratch Test): Ask the patient
to place their hand behind their back, and instruct them to reach as high
up their spine as possible. Note the extent of their reach in relation to
the scapula or thoracic spine. They should be able to reach the lower border
of the scapula (~ T 7 level).

- Abduction and External rotation: Ask the patient to place their
hand behind their head and instruct them to reach as far down their spine
as possible. Note the extent of their reach in relation to the cervical spine,
with most being able to reach ~C 7 level.

- Forward flexion: Ask the patient to trace out an arc while reaching
forward (elbow straight). They should be able to move their hand to a position
over their head. Normal range is 0 to 180 degrees.

- Extension: Ask the patient to reverse direction and trace an arc
backwards (elbow straight). They should be able to position their hand behind
their back.

Passive ROM
If there is pain with active ROM, assess the same movements with passive ROM. Have the patient relax and place one of your hands on their shoulder. Gently grasp the humerus in your other hand and move the shoulder through the range of motions described above. Note if there is pain, and if so which movement(s) precipitates it. Also note if you feel crepitus with the hand resting on the shoulder.
Pain/limitation on active ROM but not present with passive suggests a structural problem with the muscles/tendons, as they are firing with active ROM but not passive. Crepitus suggests DJD. Limitations in movement in any of the directions should be noted. Where exactly in the arc does this occur? Is it due to pain or weakness? How does it compare with the other side? Determining the precise etiology can be defined using the tests below, though realize that there is often a significant amount of overlap between several conditions.
Impingement, Rotator Cuff Tendonitis and Sub-Acromial Bursitis
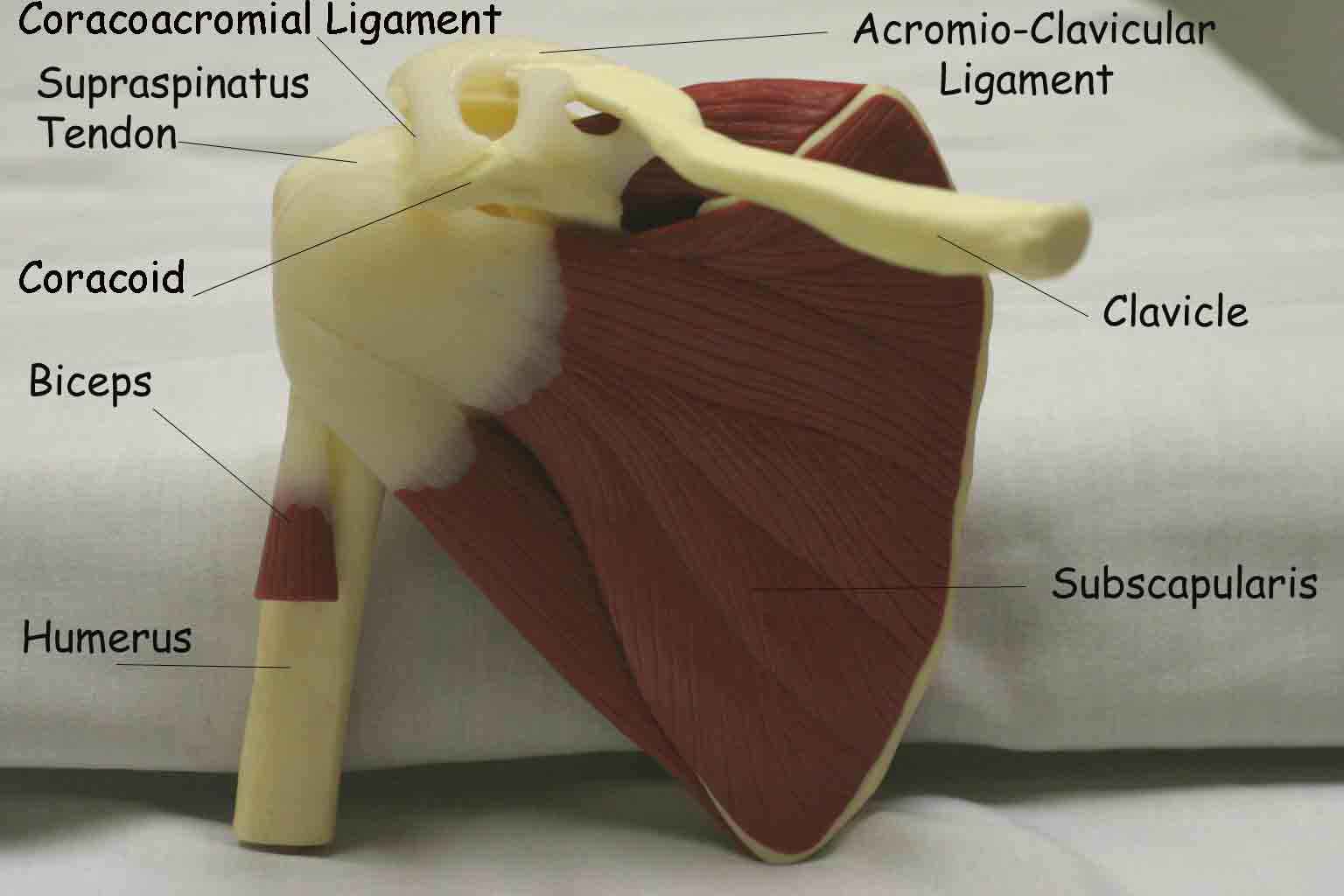
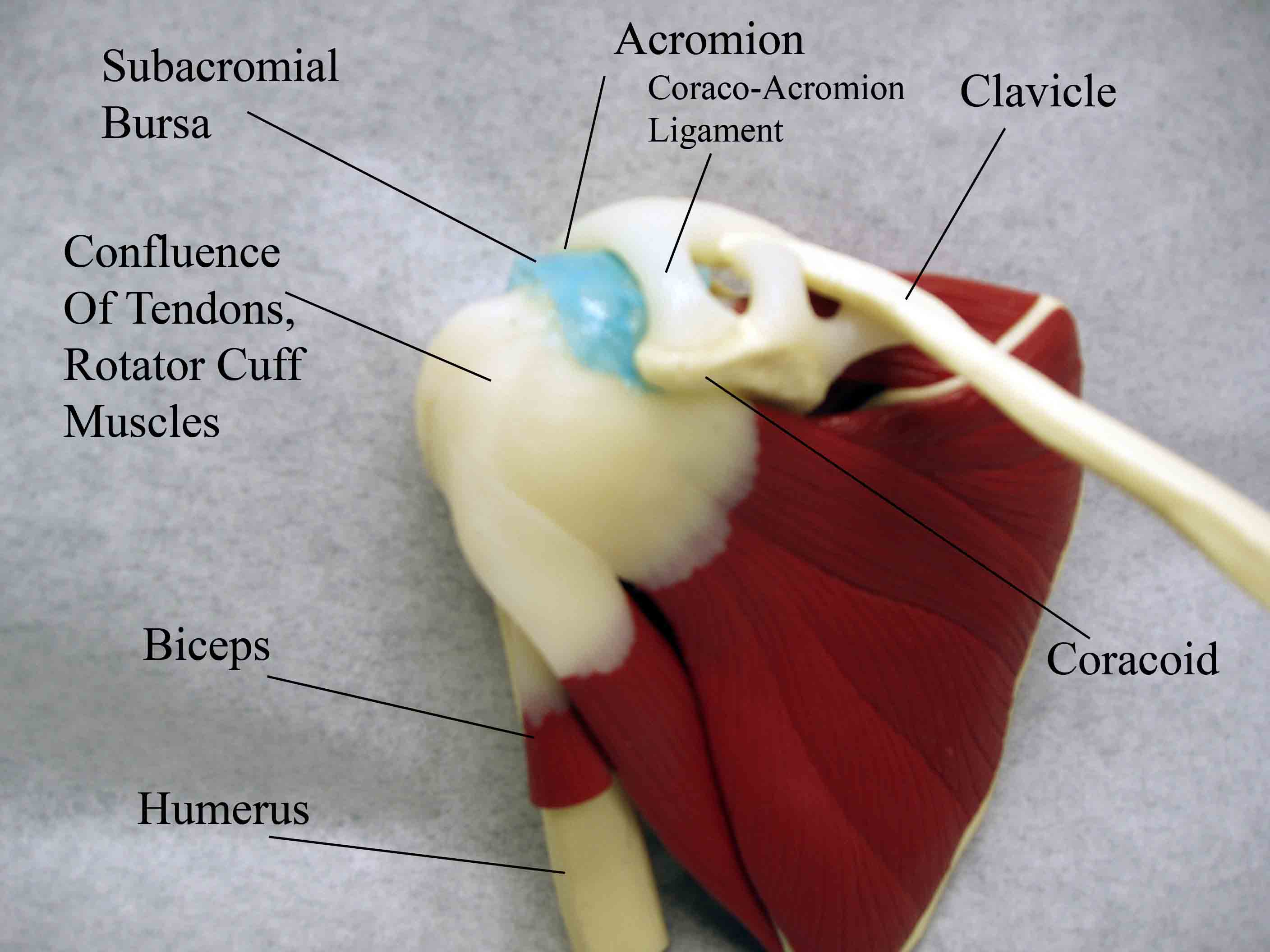
Anatomy and Function: I have placed these processes under one heading as they are all linked. Impingement is a dynamic condition that can lead to tendonitis and bursitis. Shoulder pain in general is very common, with impingement as the root cause in a large number of cases. The 4 tendons of the rotator cuff all pass underneath the acromion en route to their insertions on the humerus. The space between the acromion/coracoacromial ligament and the tendons (in particular, the supraspinatus) can become relatively narrowed for any number of reasons (e.g. the growth of an oteophyte on the under surface of the bone). This causes the tendons to become "impinged upon." The resulting friction inflames the tendons as well as the subacromial bursa, which lies between the tendons and the acromion. The net result is shoulder pain, particularly when raising the arm over head (e.g. swimming, reaching for something on a top shelf, arm positioning during sleep). Over time, chronic irritation to the tendons can lead to fraying, tears, and even complete disruption.
Several tests can be done to localize the problem:
Sub-acromial Palpation: First, identify the acromium by walking your fingers along the spine of the scapula until you reach its lateral endpoint, which is the acromium. Then gently palpate in the region of the sub-acromial space (see picture below). Palpation may cause pain if the tendons/bursa are inflamed.

The following two tests passively maneuver the tendons so that they are most likely to rub against the acromion, generating symptoms related to impingement if it is in fact present.
Neers Test:
- Place one of your hands on the patient's scapula, and grasp their forearm with your other. The arm should be internally rotated such that the thumb is pointing downward.
- Gently foreard flex the arm, positioning the hand over the head.
- Pain suggests impingement.
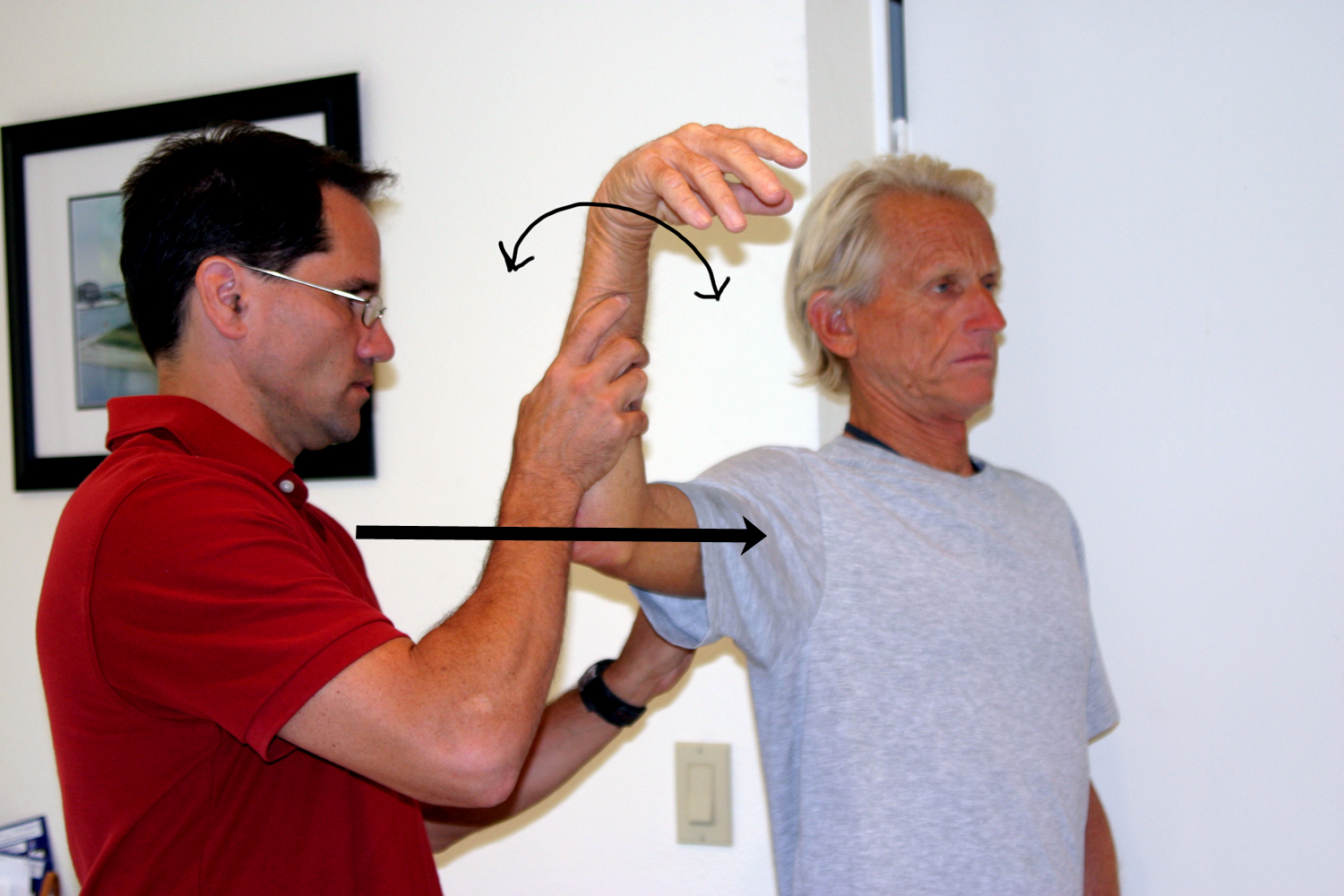
Hawkin's (for more subtle impingement)
- Raise the patient's arm to 90 degrees forward flexion. Then rotate it internally (i.e. thumb pointed down). This places the greater tubercle of the humerus in a position to further compromise the space beneath the acromion.
- Pain with this maneuver suggests impingement.

It's worth noting that defining the precise location of the problem (ie. bursitis, tendonitis or even partial rotator cuff tears) can be difficult to make on clinical grounds. One helpful adjunct is the diagnostic subacromial bursa injection. Local anesthetic and steroids are injected into the bursa. If the symptoms are due to bursitis, this provides significant relief. However, if the symptoms are predominantly caused by tendonitis or a partial rotator cuff tear, this will have little effect. MRI can also be extremely helpful in defining the precise nature of the pathology.
Evaluation of the Muscles of the Rotator Cuff
Anatomy and Function: There are 4 major muscles that allow shoulder movement. As mentioned above, symptoms caused by rotator cuff tears or tendonitis are often related to impingement. Acute shoulder trauma can also result in injury. Each of the 4 muscles can be tested individually as follows:
Supraspinatus: Connects the top of the scapula to the humerus. Contraction allows the shoulder to abduct. This is the most commonly damaged of the rotator cuff muscles. Testing (aka "empty can" test):
University of Washington, Supraspinatus
- Have the patient abduct their shoulder to 40 degrees, with 30 degrees forward flexion and full internal rotation (i.e. turned so that the thumb is pointing downward). This position prevents any contribution from the deltoid to abduction.
- Direct them to forward flex the shoulder, without resistance.
- Repeat while you offer resistance.

Interpretation: If there is a partial tear of the muscle or tendon, the patient will experience pain and perhaps some element of weakness with the above maneuver. Complete disruption of the muscle will prevent the patient from achieving any forward flexion. These patients will also be unable to abduct their arm, and instead try to "shrug" it up using their deltoids to compensate.
Infraspinatus: Connects the scapula to the humerus. Contraction allows the arm to rotate externally. Specifics of testing:
- Have the patient slightly abduct (20-30 degrees) their shoulders, keeping both elbows bent at 90 degrees.
- Place your hands on the outside of their forearms.
- Direct them to push their arms outward (externally rotate) while you resist.
Interpretation: Tears in the muscle will cause weakness and/or pain.

Teres Minor: Connects the scapula to the humerus. Provides the same function as the infraspinatus (external rotation). Testing is done as described for the Infraspinatus.
Subscapularis: Connects the scapula to the humerus, though the origin is on the anterior surface of the scapula (i.e. on the side opposite the origin of the other 3 muscles of the RC). Contraction causes internal rotation. Function can be tested using "Gerber's lift off test:"
University of Washington, Subscapularis
- Have the patient place their hand behind their back, with the palm facing out.
- Direct them to lift their hand away from their back. If the muscle is partially torn, movement will be limited or cause pain. Complete tears will prevent movement in this direction entirely.

Drop Arm Test for Supraspinatus Tears: Adducting the arm depends upon both the deltoid and supraspinatus muscles. When all is working normally, there is a seamless transition of function as the shoulder is lowered, allowing for smooth movement. This is lost if the rotator cuff as been torn. Specifics of testing:
- Fully abduct the patient's arm, so that their hand is over their head.
- Now ask them to slowly lower it to their side.
- If the suprapinatus is torn, at ~ 90 degrees the arm will seem to suddenly drop towards the body. This is because the torn muscle cant adequately support movement thru the remainder of the arc of adduction.
Deltoid: Not a muscle of the rotator cuff, but important for the later aspects of abduction and flexion. The supraspinatus is responsible for the early component of abduction. The deltoid is readily visible on exam and not commonly injured.
University of Washington, Deltoid Anatomy
Acromioclaviular Arthritis Anatomy and Function: The A-C joint is minimally mobile. However, inflammation and degeneration can occur, causing pain. Specifics of Testing:
- Identify by palpation the point at which the end of the clavicle articulates with the acromion.
- Gently push on the area, noting if it causes pain similar to what the patient was describing.
- Ask the patient to move their arm across their chest. This stresses the a-c joint and will cause pain in the setting of DJD.


AC Disruption: Trauma can cause disruption of the ac joint, also known as AC separation. Specifics of testing:
- Look at the area in question. If
there has been significant disruption (or a fracture to the clavicle itself),
the area will appear swollen and deformed compared with the other side. The patient
will avoid movement, as this causes pain.

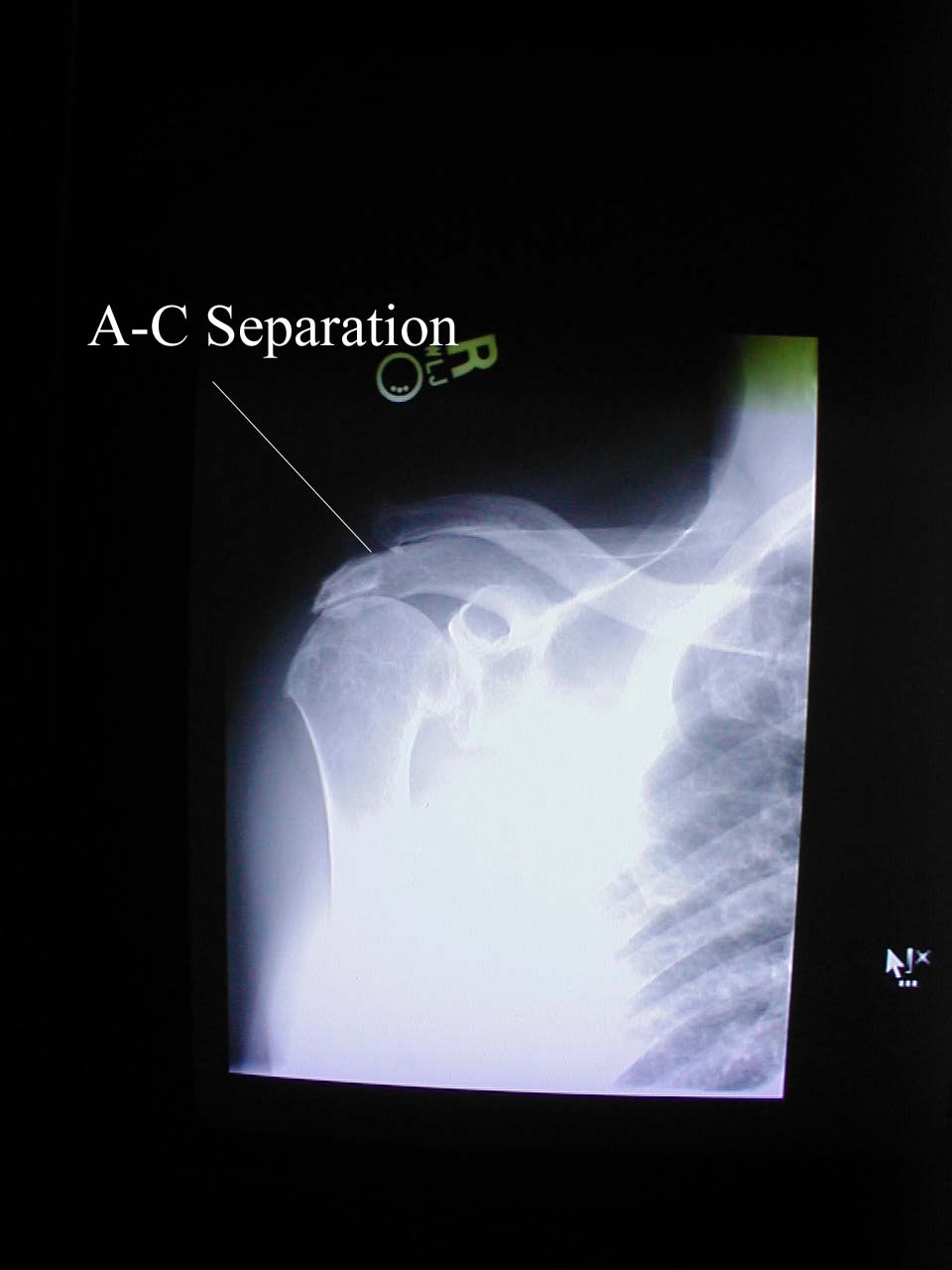 Acromio-clavicular Joint Separation: Disruption of the right A-C joint, in this case caused by trauma.
Acromio-clavicular Joint Separation: Disruption of the right A-C joint, in this case caused by trauma. - Gently have the patient move their arm across their chest while you palpate in the AC region. This will cause pain specifically at the AC joint if there is separation.
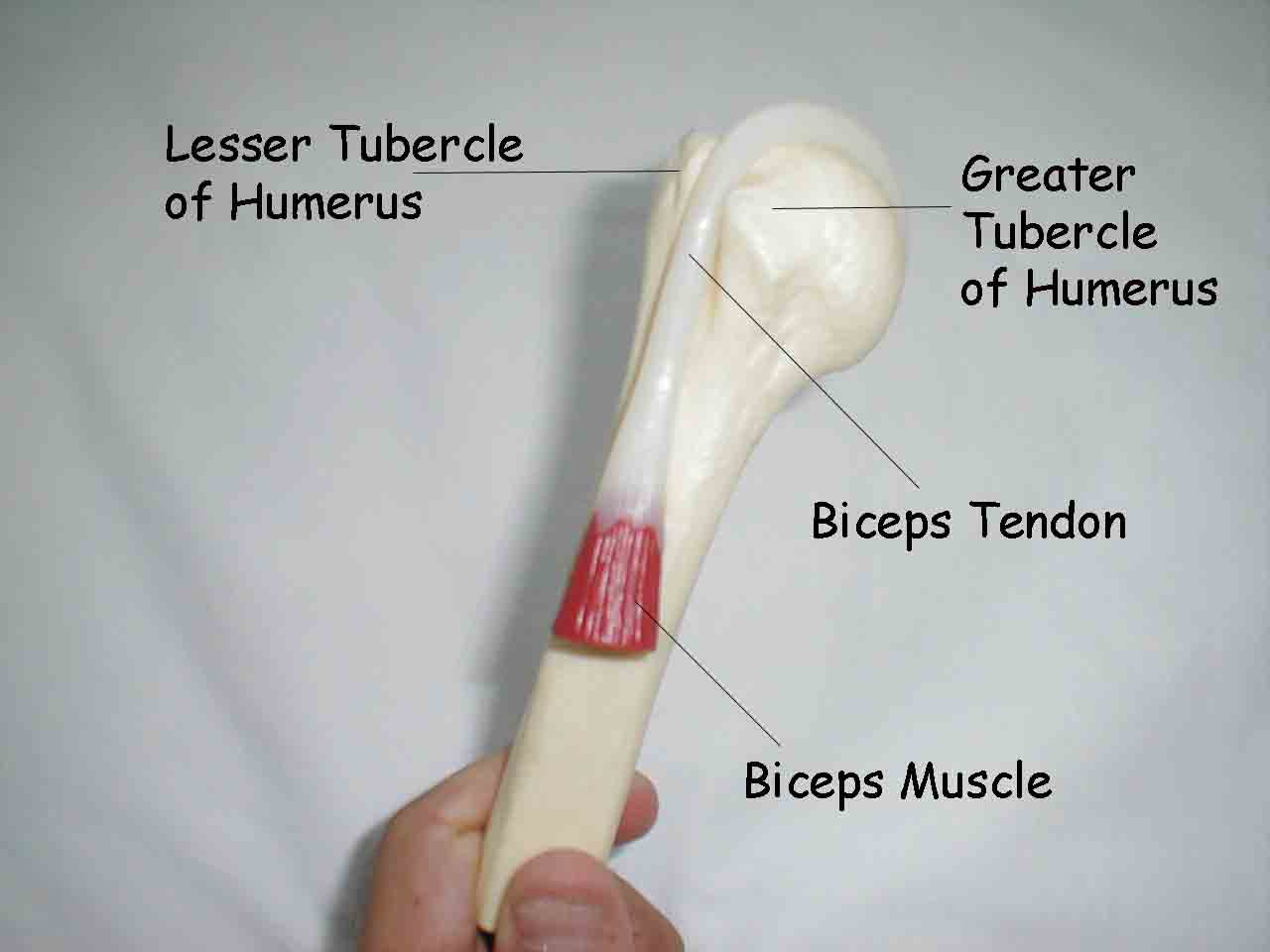
Biceps Tendonitis: The long head of the biceps tendon inserts on the top of the glenoid. The biceps muscle flexes and supinates the forearm and assists with forward flexion of the shoulder. Inflammation can therefore cause pain in the anterior shoulder area with any of these movements.
University of Washington, Biceps
Specifics of testing:
- Palpate the biceps tendon where it sits in the bicipital groove, which is formed by the greater and lesser tubercles of the humeral head. Pain suggests tendonitis. It helps to have the patient externally rotate their shoulder. You can confirm the location of the tendon by asking the patient to flex and supinate their forearm while you palpate, which should cause it to move.

Resisted Supination (Yergason's Test):
- Elbow should be flexed to 90 degrees, shoulder adducted (ie elbow bent at right angle, arm against body).
- Grasp the patient's hand and direct them to try and rotate their arm such that the hand is palm up (supinate) while you provide resistance. Pain suggests tendonitis of the biceps.

Speed's Maneuver for Bicipital Tendonitis:
- Ask the patients to position the affected arm such that the elbow is flexed to ~30 degrees and the forearm supinated (palm up).
- Direct the patient to flex their arm as you provide resistance. In the setting of tendonitis, this will produce pain.
Biceps Tendon Rupture: As a result of chronic tendonitis or truama, the long head of the biceps may rupture. When this occurs, the biceps muscle appears as a ball of tissue and there is a loss of function.

The Glenohumeral Joint
Anatomy and Function: This joint is the actual place where the humerus articulates with the scapula (i.e. where the ball meets the socket). The cavity is lined by the labrum, which functions like the menisci of the knee, assuring smooth/cushioned contact between the bones. The joint is held together by the muscles of the rotator cuff as well as a tough capsule that surrounds the muscles.
Glenohumeral DJD: DJD usually results from an injury that has disrupted the normal articulating surfaces. Over time, movement of the shoulder causes additional wear and tear, leading to DJD. Patients experience pain and gradual limitation in movement. This is particularly noticeable on external rotation and abduction. Palpation of the joint with a hand placed on the shoulder during movement may reveal crepitus. Assessment is done as follows:
- Perform active ROM maneuvers as described previously, noting degree to which movement is limited.
- Perform passive ROM, again noting limitations and degree of pain.
- You may feel crepitus by placing your hand on the patient's shoulder during passive ROM.
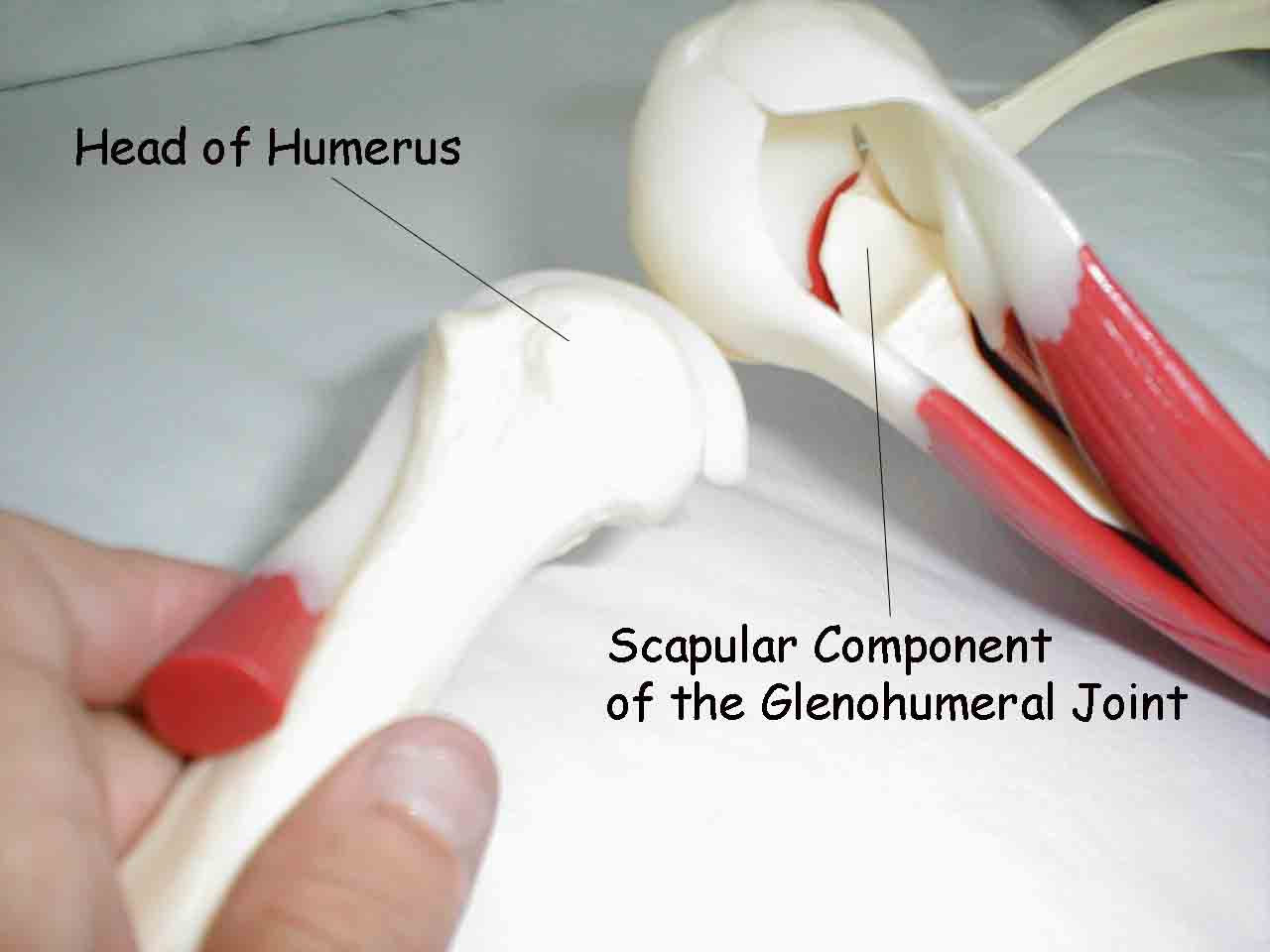
Glenohumeral Instability: The rotator cuff, along with the outer joint capsule and the labrum, stabilize the joint. The labrum is a tough tissue that lines the cup formed by the scapular component of the glenohumeral joint. The rotator cuff and capsule surround the outside of the joint. Together, they allow the humerus enough freedom so that the shoulder maintains its full range of motion and function. Tears of the capsule or labrum can generate feelings of pain, instability, or a "dead arm" sensation. The patient may have a history of trauma or recurrent dislocation, where the humerus actually pops out of joint. Specifics of testing (The Apprehension Test):
- Have the patient lie on their back with the arm hanging off the bed.
- Grasp their elbow in your hand and abduct the humerus to 90 degrees.
- Gently externally rotate their arm while pushing anteriorly on the head of the humerus with your other hand.
- Instability will give the sense that the arm is about to pop out of joint.

- Patient supine.
- Push on the humerus in posterior direction while externally rotating the arm.
- This maneuver should relieve any feeling of pain and/or sense that the shoulder
is going to dislocate.
Note, this technique is essentially the opposite of that used for the aprehension test.
Crank Test (For Labral Injury)
- Patient's arm is abducted and elbow flexed.
- Examiner directs humerous into glenohumeral joint while at the same time rotating the arm.
- Pain elicited during this maneuver suggests labral tear.
Obrien's Test (For Labral Injury)
- Patient's arm abducted to 90 degrees, forward flexed to 90 degrees, then positioned across the chest, towards the opposite shoulder.
- Hand positioned so thumb is pointing down.
- Examiner resists as the patient tries to raise their arm
- Pain suggests that there is a labral injury
- Repeat the test, with the patient's thumb pointing up. Less pain in this position is further suggestive of an injured labrum.
Acute Inflammatory Arthritis: Inflammatory processes within the joint can be caused by a number of processes, including infection (septic) or autoimmune (e.g RA). When this occurs, the shoulder may appear swollen, red, and will be painful to the touch. Any movement will be limited by pain. Sampling of fluid from within the joint space allows definitive diagnosis.


Adhesive Capsulitis: Also called a frozen shoulder, this is caused by idiopathic inflammation of the capspule around the shoulder. The net result is severe limitation of motion in any direction (active or passive). Pain is present with movement, and oftentimes when the shoulder is at rest. The etiology is unclear and it can be difficult to distinguish from a number of the above conditions.
Referred Pain to the Shoulder Area
It's important to recognize that not all shoulder pain is cause by shoulder pathology. A few sites that can cause referred symptoms:
- Intra-abdominal inflammation can cause pain to be referred to the shoulder. In particular, inflammation that takes place just below the diaphragm (e.g. splenic abscess) may be referred to the shoulder. Examination and history would suggest that the pathology lies outside the shoulder.
- Intrathoracic processes can also cause referred symptoms. MI, for example, can generate pain that radiates to the shoulder. As above, H&P should be revealing.
- Cervical spine pathology can cause irritation of the cervical nerve roots, in particular C5 and C6. This causes a burning or tingling type pain to be referred to the deltoid area. Appropriately directed history and neuro examinations help to pin down the cervical spine as the location of the pathology.