Musculo-Skeletal Examination
Elbow
Function and Anatomy:
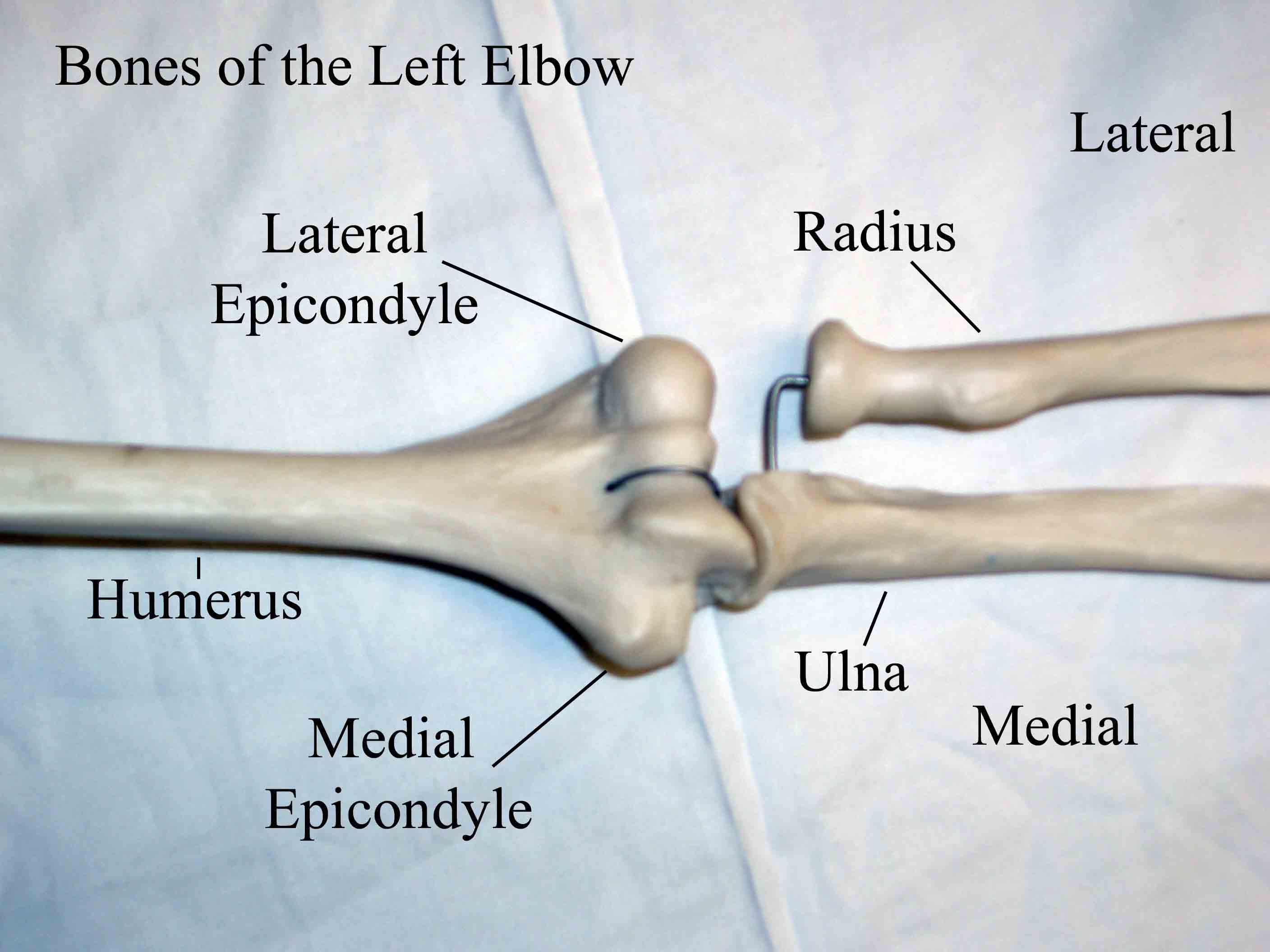
Hinge type joint formed by the articulation of the Ulna and Radius (bones of the forearm), and Humerus (upper arm). Full extension is equal to 0 degrees, full flexion to ~ 150 degrees. Maximum supination (turning hand palm up so that it can hold a bowl of "soup") and pronation (palm down) are both 90 degrees.
For Additional Information See: Digital DDx: Elbow Pain

Elbow Pain and Symptom Syndromes
- Lateral Epicondylitis (tennis elbow):
Presentation and Anatomy: Extensors and supinators of the wrist insert on the lateral epicondyle of the humerus. Repetitive extension (e.g. back hand motion in tennis, though could be any activity with similar movement) of the wrist can cause inflammation and pain around this bony prominence. Examination is usually remarkable for:- Pain on palpation around the lateral epicondyle.
- Reproducibility of pain with resisted wrist extension and supination.
- Absence of warmth, erythema, or other findings of acute inflammation.
 Palpation of lateral epicondyle
Palpation of lateral epicondyle Resisted Wrist Extension
Resisted Wrist Extension - Medial Epicondylitis (golfer's elbow): Presentation: Flexors and
pronators of the wrist insert on the medial epicondyle. Repetitive flexion
of the wrist can cause inflammation and pain around this bony prominence.
Examination is usually remarkable for:
- Pain on palpation around the medial epicondyle.
- Reproducibility of pain with resisted wrist flexion.
- Absence of warmth, erythema, or other findings of acute inflammation.
 Palpation Medial Epicondyle
Palpation Medial Epicondyle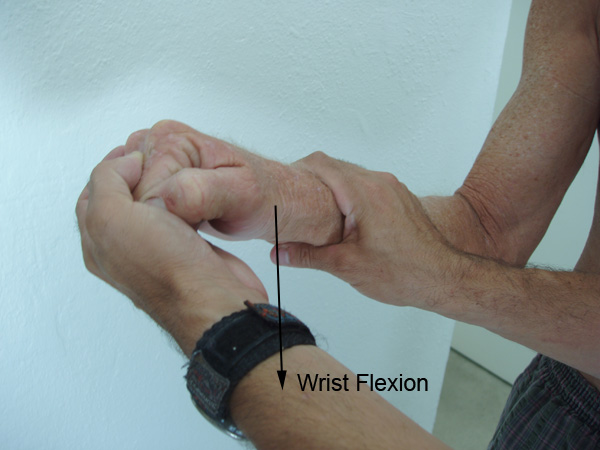 Resisted Wrist Flexion
Resisted Wrist FlexionHelpful Hint: If you forget where the flexors and extensor insert, extend and flex your own wrist while palpating both epicondyles with the other hand. It will become clear that your extensors attach laterally and flexors medially.
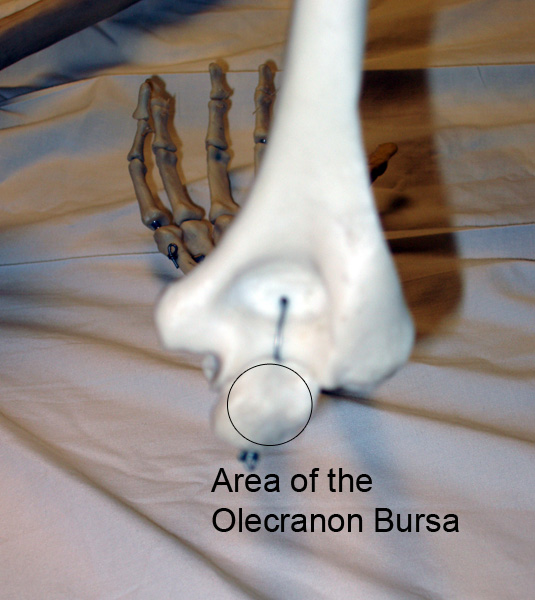
- Olecranon Bursitis Anatomy: The olecranon process is formed by the
proximal aspect of the Ulna and is the bony prominence that forms the tip
of the elbow. The olecranon bursa is a fluid filled pouch that is located
directly on top of the olecranon process. It provides a lubricating pad that
minimizes direct trauma to the underlying bone during usual activity. Normally,
the bursa is not apparent on examination. There are several situations when
it becomes clinically prominent:

- Non-Inflammatory Bursitis
Presentation:
As a result of repeated trauma (e.g. persistent leaning on elbows), excess fluid can develop within the bursa, causing it to become very apparent on direct observation. Examination is remarkable for:- Obvious swelling at the tip of the elbow.
- Absence of pain, redness or warmth, as there is usually a minimum of inflammation.
- Full, painless range of motion of the elbow.
 Normal Elbow
Normal Elbow Minimally Inflammatory Olecranon Bursitis
Minimally Inflammatory Olecranon Bursitis - Inflammatory Bursitis
Presentation and Anatomy: As a result of infection (via abrasion to overlying skin) or any other intensely inflammatory process (e.g. gout, rheumatoid arthritis), the bursa can become very inflamed. Examination in this case is remarkable for:- Obvious swelling at the tip of the elbow
- Marked warmth, redness, and pain on palpation of the bursa.
- Range of motion of the elbow is usually preserved. This is one way of distinguishing inflammatory bursitis from inflammatory arthritis. Infection within the elbow joint (inflammatory arthritis) is rather rare. When it occurs, the elbow area is diffusely swollen (ie not limited to the area of the bursa) and there is pain with any flexion or extension of the elbow. Rarely, bursitis and/or cellulitis can be so severe that ROM is compromised, making it difficult to distinguish these entities from intra-articular inflammation.
- Non-Inflammatory Bursitis


- Ulnar Nerve Entrapment
Presentation and Anatomy: The ulnar nerve runs in the groove between the medial epicondyle and olecranon process. When inadvertently struck, it causes the "funny bone" sensation of pins and needles/electric shock traveling down towards your hand. The ulnar nerve provides sensation to the pinky and medial half of the ring finger. It also provides motor function that allows wrist flexion (along with the median nerve), finger flexion (grip), finger adduction and finger abduction. Occasionally, pressure can develop on the nerve due to entrapment as it travels around the elbow. When this occurs, patients report neuropathic type pain (pins and needles, electric shock) along the nerve's distribution (i.e. from elbow down to the hand; sometimes also migrating proximal to the elbow).Examination in the setting of ulnar entrapment:
- Normal external appearance
- Usually normal motor strength: wrist flexion, finger flexion (grip), finger adduction/abdution. May be compromised if nerve compression is severe and of long duration.
- Usually normal sensation in the pinky and medial half of the ring finger (assess by checking 2 point discrimination).
- Pain reproducible with tapping over nerve, referred to as ulnar Tinnel's
sign.
 Ulnar Tinnel Test
Ulnar Tinnel Test