Musculo-Skeletal Examination
Hip
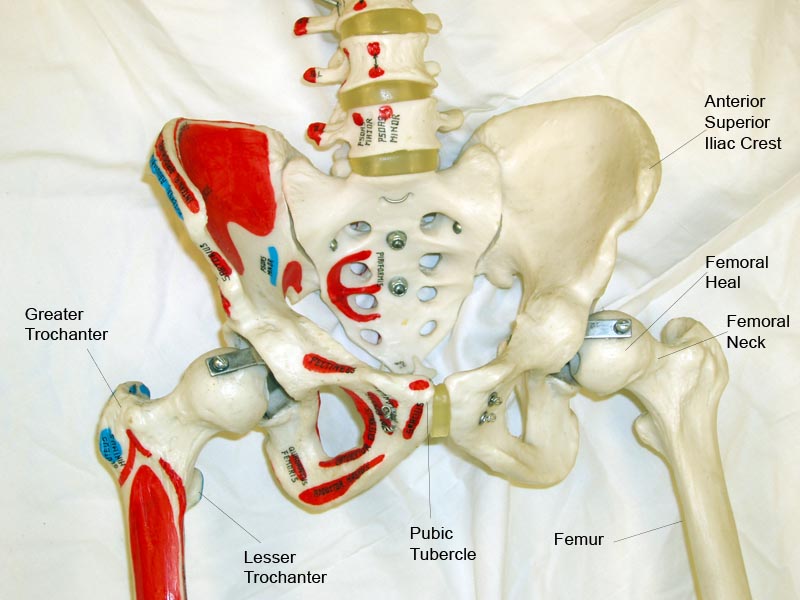
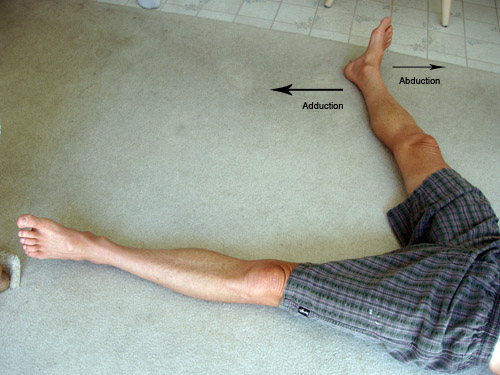
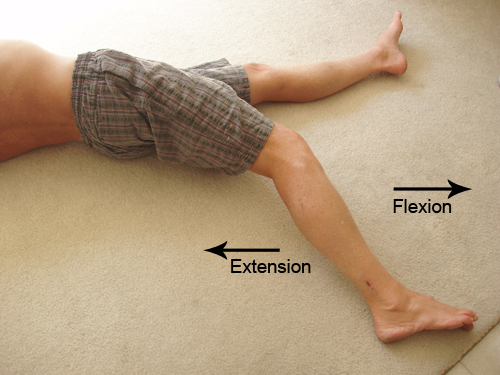
Function and Anatomy: The hip is a ball and socket type joint, formed by the articulation of the head of the femur with the pelvis. Normal range of motion includes: abduction 45 degrees, adduction 20-30 degrees, flexion 135 degrees, extension 30 degrees, internal and external rotation. Hip pathology can cause symptoms anywhere around the joint, though frequently pain is anterior and radiates to the groin region. Additionally, pathology outside of the hip can be referred to this region. History and exam obviously help in making these distinctions.
For Additional Information See: Digital DDx: Hip Pain
A few common problems are described below:
- Degenerative Joint Disease and Osteoarthritis
Presentation and anatomy: Patients usually report pain with weight bearing and ambulation. Symptoms progress slowly over time (ie years) with pain precipitated by less activity (ie shorter distances walked) as the disease worsens. This tends to occur in patients > 50, as age increases the risk of wear and tear on the joint. Obesity, which chronically increases the load and stress that the joint must bear, is a major risk factor. There may also be a history of significant antecedent trauma that damaged the joint, "setting it up" for degenerative changes over time.
Examination:
- Pain with walking, perhaps even with limping. Patient's may develop an Antalgic gait, characterized by trying to minimize the amount of time spent with weight bearing on the affected joint.
- Range of motion reduced as degeneration progresses. Early on, internal rotation may elicit more pain then movement in other directions.
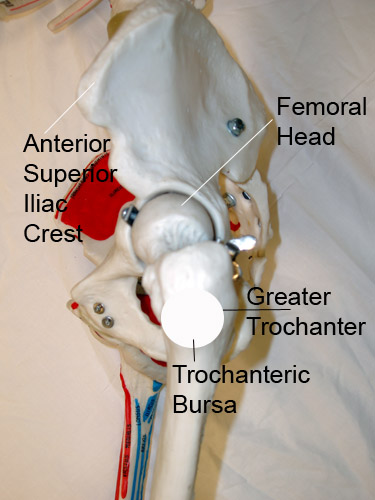
- Trochanteric Bursitis:
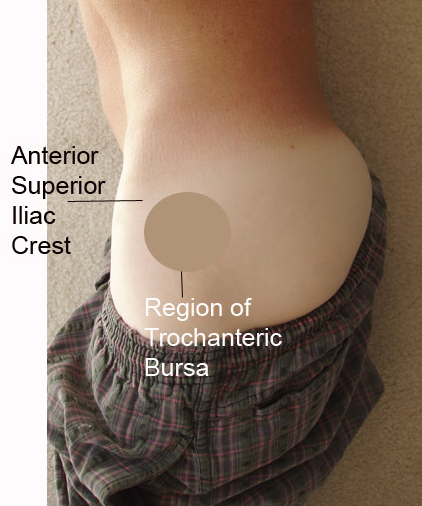
Anatomy and function: The troachanteric bursa overlies the greater trochanter of the femur. When it becomes inflamed, patient's report vague hip pain, focused on the lateral area of the joint. Symptoms tend to get worse with walking.
Examination:
- Range of motion is generally preserved
- Pain on direct palpation over the bursa
- Pain with resisted abduction. This can be assessed by having patient lie on unaffected side and asking them to abduct the affected hip as you provide resistance.